Parkland Center for Clinical Innovation releases its 2025 annual impact report highlighting recent accomplishments
Parkland Center for Clinical Innovation (PCCI), a non-profit innovation and research institute for advanced data science and non-medical drivers of health (NMDoH) innovation, has released its annual impact report detailing its successes and activities from 2024.
“The Annual Impact Report features some of the outstanding results the team at PCCI had in 2024,” said Steve Miff, PhD, President and CEO of PCCI. “The report highlights our expanding AI in medicine for underserved populations solutions through novel programs and partnerships in North Texas and around the state.”
These AI-focused programs featured in the report include PCCI’s leadership in advanced AI and NMDoH analytics for clinical decision support and population health and surveillance systems. The report also features the national activities and engagements of PCCI experts and leaders who drive the organization’s programs and mission to support the underserved.
“I am very excited to share the accomplishments and leadership of our team and our partners,” Miff said. “Our mission of driving innovation in AI for underserved populations is at the heart of everything we do. This past year our team built and deployed novel and scalable solutions and contributed to the emerging knowledge and guidelines for ethical, responsible and equitable uses of AI in healthcare.”
The Parkland Center for Clinical Innovation (PCCI) is a not-for-profit, mission-driven organization with industry-leading expertise in the practical applications of artificial intelligence, machine learning and NMDoH data modeling to address the needs of vulnerable populations. PCCI started as a department within Parkland Health and was spun out as an independent organization in 2012. PCCI strives to leapfrog the status quo by harnessing the transformative potential of data. Our unique capabilities allow us to provide innovative, actionable solutions that more effectively identify needs, prioritize services, empower providers, and engage patients.
Disparities Next Door: PCCI’s Community Vulnerability Compass spotlights areas of increased vulnerability across Dallas County
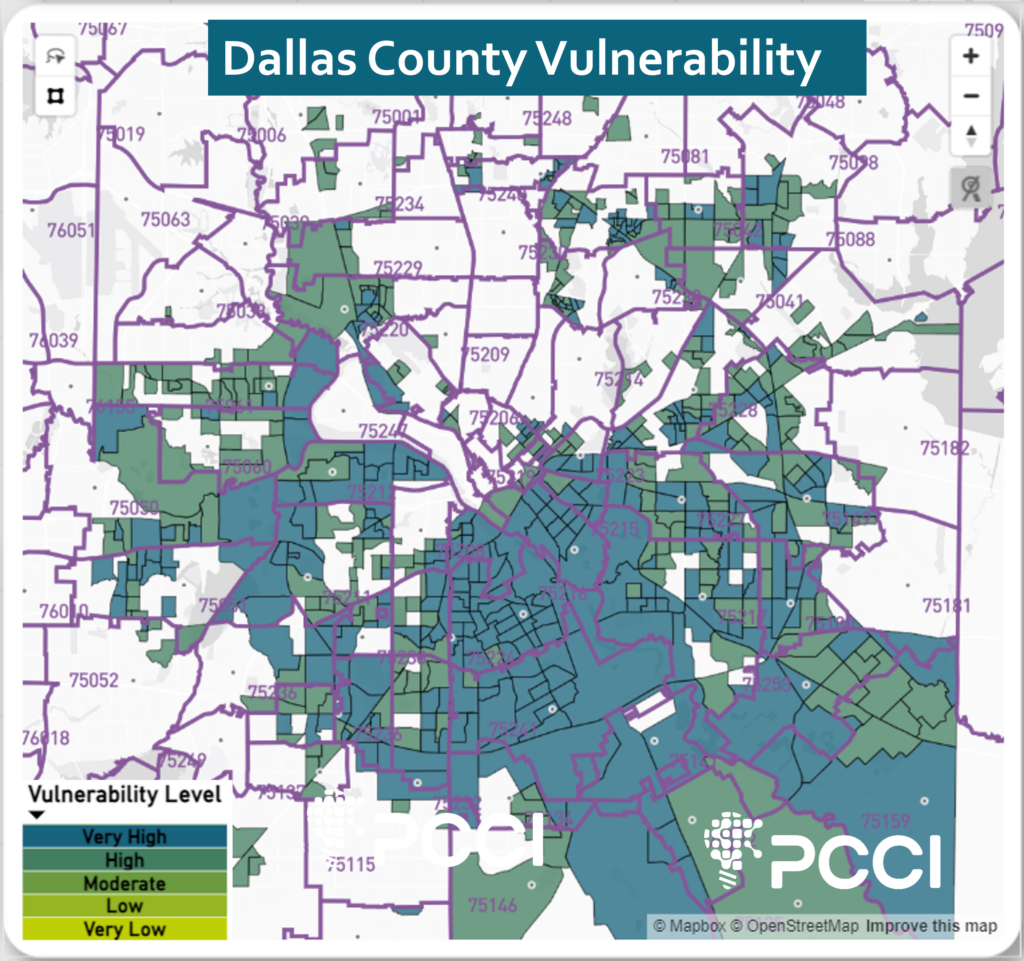
Dallas, Texas(Sept. 19, 2024) – Researchers at Parkland Center for Clinical Innovation (PCCI) have highlighted areas of increased vulnerability within Dallas County after conducting an analysis using PCCI’s Community Vulnerability Compass (CVC). The findings include a number of pockets of highly vulnerable areas within many low vulnerability ZIP Codes.
PCCI’s CVC analyzes, at the ZIP Code, census tract, and block-group level, where a community’s most vulnerable residents live and the root cause factors limiting these residents’ ability to thrive. The CVC analyzes 26 clinical and socio-economic indicators that reveal the health, resiliency, and economic vibrancy of neighborhoods. CVC’s analyses provide true, holistic pictures of who needs the most assistance and where to find them, enabling proactive support of those in need.
It is well-documented that many ZIP Codes in the south and southeast areas of Dallas County (see image 1) are home to long-standing socio-economically disadvantaged populations and have the highest vulnerability rating. However, PCCI’s analysis underscores what Parkland and other officials have long stated: that in addition to the south and southeast regions, there are other ZIP Codes in Dallas County with low vulnerability but are home to highly vulnerable block groups. Specifically, these include 18 Dallas County ZIP Codes with an overall very low or low vulnerability rating that contain within them 48 block groups with high or very high vulnerability ratings. The 18 ZIP Codes have a total population of 590,971, with 72,954 (12.3%) of their residents living in these very high vulnerability blocks groups.
“In some cases, we find that a very high area of vulnerability is across the street from a very low area of vulnerability.“
Steve Miff, phd, President and CEO of PCCI
The “very high” designation indicates that these neighborhoods are in the top 20% of vulnerability when compared to the rest of Dallas County. CVC vulnerability groupings are localized to the Dallas County geography and broken into quintiles and clustered into very low, low, moderate, high and very high areas.
“For good reason we focus a lot of our efforts on supporting the underserved communities in south and southeast Dallas County, but CVC empowers us with refined geographic precision to examine our broader community and uncover data that provides a high-resolution understanding of social vulnerability factors within other micro-geographies in our community,” said Steve Miff, PhD, President and CEO of PCCI. “In this examination, CVC highlights areas of deprivation that may be masked by gentrification and/or historical surrounding prosperity. In some cases, we find that a very high area of vulnerability is across the street from a very low area of vulnerability.”
For example, ZIP Code 75206, located in the Greenland Hills area that runs along Highway 75 and is bordered by Highway 12 and Skillman Avenue, is rated very low vulnerability by the CVC, but includes four block groups that are rated by the CVC as high and very high vulnerability. In this ZIP Code, which has a total population of 38,209, there are 2,661 (7%) who experience high or the very highest levels of vulnerability as measured by the CVC.
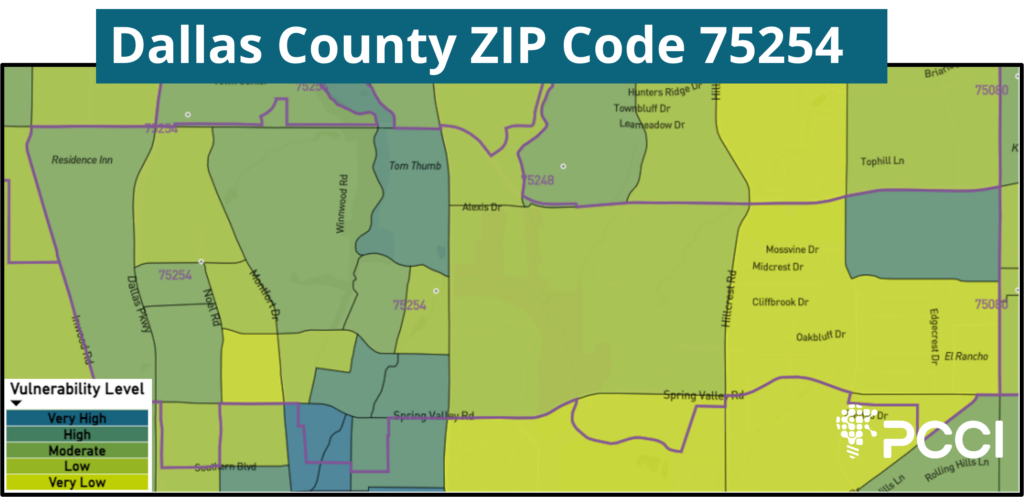
One ZIP Code of note, 75254, located north of the Galleria between Dallas North Tollway and Coit Road, has an overall low vulnerability rating, but includes 8 high or very high vulnerability blocks. Of this area’s total population of 24,047, 12,522 (52.1%) residents experience high or very high vulnerability. (see Image 2)
Additionally, ZIP Code 75230, which is considered to be an economically advantaged area in North Dallas between Walnut Hill and Interstate 635, includes a very high vulnerability block group.
“The lesson is that we need to look beyond our expectations and understand that disparities and vulnerability are all around us no matter how prosperous a given area may appear,” Miff said. “We hope this will bring an additional level of high-resolution, hyper-localized understanding of social vulnerability factors and empower leaders across all communities with relevant information to improve and sustain the lives of all Dallas County residents. North Texas has outstanding public health leaders who are doing a great job supporting vulnerable populations throughout the county and we hope this helps them as well as policymakers, community-based organizations and others who are vested in helping mitigate disparity.”
IMAGE 1
IMAGE 2
About PCCI
The Parkland Center for Clinical Innovation (PCCI) is a not-for-profit, mission-driven organization with industry-leading expertise in the responsible application of artificial intelligence, machine learning and NMDOH data modeling to address the needs of vulnerable populations. PCCI started as a department within Parkland Health and was spun out as an independent organization in 2012. PCCI strives to leapfrog the status quo by harnessing the transformative potential of data. Our unique capabilities allow us to provide innovative, actionable solutions that more effectively identify needs, prioritize services, empower providers, and engage patients.
AI Is Working For Us Now, Helping Us Heal and Prevent Harm
By Steve Miff, PhD, President & CEO of PCCI
We can’t let artificial intelligence (AI) continue to be defined by science fiction, deep fakes, and plagiarized term papers, because today―right now― responsible uses of AI in medical care are helping prevent harm, improve clinical decisions, and reduce costs of care. Is there too much unjustified hype and exuberance over AI? Absolutely! Are there unsubstantiated claims and sometimes dangerous promises? Unfortunately, yes. However, there are also many examples of ethical, responsible and equitable uses of AI that are streamlining operations, improving efficiencies, and yes, even helping physicians and clinical teams augment their insights and expertise to save lives.
AI is also not new. While the history of artificial intelligence (AI) can be traced to antiquity hypothesized by master craftsmen, modern AI really started with the invention of the programmable digital computer based on mathematical reasoning in the 1940s. In the last decade, the true potential (and risk) of AI and Machine Learning algorithms have accelerated and can simply be classified into predictive, prescriptive and generative AI/ML, with the latter creating the most excitement and controversy over the last 12-24 months.
At PCCI, we have been researching, developing, deploying and testing applications of AI and machine learning for a decade with a focus on applying these innovative concepts to those who serve the most vulnerable individuals and communities. With every project that we’ve embarked on, we’ve followed sound scientific principles and a prescriptive approach to development, testing and implementation that keeps the clinician in full control and with the utmost transparency, and the patient at the center. While the AI part is sexy, the governance, processes, and discipline you put around it makes it reliable, responsible and effective. We developed and optimized our own processes over type and rely on a core set of core principles:
There needs to be a clearly articulated problem and need that the AI is trying to solve/augment. If you don’t have a real problem to solve, it’s just cool math.
A multi-disciplinary team that includes an engaged and passionate lead clinician is required from day 1. The front-line staff already have the knowledge and intuition of what is needed and what could work.
More than half the time is spent on ensuring data quality and staging – researching, curating, studying, aggregating, ingesting, validating, augmenting and analyzing data from multiple sources is the lifeblood of any successful model. The old saying of “junk in, junk out” is even more crucial with AI.
Focus just the data required for the initial development, but understanding the required data latency, refresh frequency, storage and compute requirements to understand deployment requirement and cost to operationalize and sustain.
You need your own AI sandbox and your EHR is not it. PCCI developed Isthmus™, a secure, digital data environment leveraging established cloud technology and optimizing open-source tolls for end-to-end, secure data orchestration, modeling and deployment.
Data security is paramount, hence why PCCI deploys Isthmus™ within the firewalls of a health system/payer/provider (no protective data is moving out)
There is a prescriptive stage-gate development and deployment process that requires patience and time:
Build models leveraging historical data; T
Test the preferred model with a reserved data set
Optimize the performance of the model leveraging clinician input to optimize how the model is to perform and be used in practice
Deploy the model with real-time data and run it silent mode. No decisions are made using the model, but the performance, stability, expected output is evaluated and monitored. Evaluate for equity and expected performance on the respective patient population. This could take months, or years. If you’re trying to predict a rare event, it will require extensive time to ensure adequate amount of time and data is being processed. To ensure proper evaluation for the PCCI Parkland Trauma Mortality (PTIM), we went into a full silent mode on every patient every hour for 3 full months before we moved to provider facing production.
Design the output and display of the model and integrate into the EHR or case management system where clinical teams do their work (no extra clicks or sign-on to get to the information). Integrate and deploy systems that give clinical teams insights into the metrics behind the model. PCCI developed and deployed a web-based interface called Islet™ that provides real-time insights into a model. This is critical not only to ensure transparency to clinical teams, but it’s extremely valuable to point to the top factors and the data driving the algorithms to point to the factors that can be actioned
Design a stages go-live deployment process and incrementally expend teams and/or department while evaluating each deployment
Ensure a robust and coordinate response process to address off-cycle failures. While the models are designed to augment clinical decisions, the power of AI is tangible and useful and clinical teams rely on their assistance. It’s like getting used to driving on automatic transmission car and then having to go back to driving stick. You can still drive, but it’s not as easy.
This is not a one-and-done. Far from it. Develop and stick to a regular cycle of model evaluation, testing and updates
At PCCI speed to market is a self-imposed urgency and profits are not a measure of success. What our AI and machine learning systems aim to do is help providers make more informed clinical decisions, optimize resources to expand access, offer synthesized data insights that help improve health outcomes, and educate our region’s health leaders and residents.
Some of these AI predictive model applications came to life during the COVID-19 pandemic. We were able to use the established infrastructure, processes and expertise to create several programs that made significant impact on how Dallas County managed through the pandemic. A few of these AI and predictive models included:
Capacity Forecasting Model. Leveraging an AI algorithm based on geo mapping, we helped Parkland manage resources by creating an effective model that helped forecast possible needs for hospital beds, ICU, staffing needs, and development of workflows.
Proximity Index (PI). This AI predictive triage model empowered frontline clinical and population health teams to proactively manage high-risk patients and reduce potential COVID spread from asymptomatic patients in hospital and community settings.
Vulnerability Index (VI). This AI predictive model allowed public health leaders to understand the hardest hit populations in Dallas County and then drive community response.
Beyond COVID, PCCI’s AI-driven clinical decision support and population health programs guide policy and direct resources where they are needed most. PCCI’s team members have extensive experience deploying, testing, and validating a wide array of multi-institution, algorithm-driven protocols in clinical settings. Examples include:
Parkland Trauma Index of Mortality (PTIM)
The PTIM machine learning algorithm is the only known model that uses electronic medical record data to predict ―every hour ― 48-hour mortality during the first 72 hours of hospitalization, thus evolving with the patient’s physiologic response to trauma. Over a one-year period, PTIM has correctly identified 89% of the high-risk trauma patients and 92% of the low-risk trauma patients.
Inpatient (IP) Medicine Sepsis AI Program
The sepsis management system is real-time predictive model that identifies and triggers interventions of patients who are at high risk for sepsis both upon presentation and after being admitted to the hospital. The IP Sepsis model is unique as it enables Parkland to identify cases of sepsis that were not present on admission.
STI-HIV PrEP Model
The model will be able to predict those at-risk for hiv infection and eligible for prep in order to reduce HIV transmission. The PrEP predictive model is being developed using data from Parkland’s EHR, pertinent public open-source data on NMDOH, and DCHHS STI data. The model will be able to predict those at-risk for HIV infection and eligible for PrEP to reduce HIV transmission.
Preterm Birth Prevention (PTB) AI-driven Program
To better serve pregnant women, PCCI and the Parkland Community Health Plan developed and implemented an innovative Preterm Birth (PTB) Prevention program that uses a machine learning algorithm, healthcare data, and Non Medical Drivers of Health to identify pregnant women who are at a higher risk of PTB within vulnerable communities. The PTB program consistently risk stratifies about 13,000 pregnant women from vulnerable communities per year.
Pediatric Asthma Surveillance System (PASS)
PCCI developed the PASS to help prevent pediatric asthma from harming children in Dallas by providing a single source of community insights to identify children that have higher vulnerability to poor asthma outcomes and highlight areas of health disparities. The PASS interactive dashboard has been visited by nearly 3,000 Dallas County residents.
Many of these programs have proven to be cost effective, scalable and successful. We will continue to invest and explore new ways to apply AI solutions in collaboration with some of the top healthcare providers and public health organizations in the nation.
Whether everyone knows it, understands it or even likes it, AI is here to stay and is exploding in healthcare, and making a huge difference in our lives. At PCCI we will continue to focus on applying and localizing these powerful concepts with those who serve the most vulnerable individuals and communities. That’s our mission and focus and will remain that way. This specifically means continuing our work with Parkland Health (Parkland), PCHP, Dallas County Health & Human Services Department (DCHHS), the United Way of Metropolitan Dallas, and expanding our partnerships with other similar organizations in San Antonio, Austin, Atlanta and other communities.
Because of the responsibility that has been entrusted in us, we feel the urgency and responsibility to not only continue to learn from others pioneering responsible applications of AI, but contribute to the knowledge, voice and narrative of AI nationally. That’s why we’re appreciative to be included and actively participate in national AI committees and collaboratives, such as the Health AI Partnership advisory board, the National Academy of Medicine AI Adoption and Code of Conduct committee, the White House Health AI commitments executive group, as well as several other national meetings and forums. We bring the important perspective and the unique challenges of leveraging these new and exciting capabilities in an equitable was and make these innovations accessible to underrepresented and underserved communities.
For many the promise of AI is about what’s on the horizon, but I see the promise of AI delivering results and innovations today. With responsible, equitable, reliable and transparent applications, the future is now.
About Steve Miff
Dr. Steve Miff is the President and CEO of Parkland Center for Clinical Innovation (PCCI), a leading, non-profit, artificial intelligence and cognitive computing organization affiliated with Parkland Health, one of the country’s largest and most progressive safety-net hospitals. Spurred by his passion to use next-generation analytics and technology to help serve the most vulnerable and underserved residents, Steve and his team focus on leveraging technology, data science, and clinical expertise to obtain unique non-medical-determinants-of-health data and incorporate those holistic, personal insights into point-of-care interventions. Steve was the recipient of the 2020 Dallas Business Journal Most Inspiring
University Health Transplant Institute partners with Parkland Center for Clinical Innovation to implement innovative data management to improve patient outcomes
Dallas, Texas – University Health Transplant Institute, dedicated to restoring health and life to patients with organ failure through prevention treatments and transplantation services, is partnering with the Parkland Center for Clinical Innovation (PCCI). The goal of this partnership is to improve care and outcomes by combining artificial intelligence with clinical expertise, to enhance the Transplant Institute’s digital data environment allowing for enhanced data access and advanced analytics to enable transformative innovation and high-impact research.
Currently in the implementation phase, PCCI is expanding University Health’s capabilities based on deploying PCCI’s innovative, cloud-based, digital data environment, ISTHMUSTM, and leveraging PCCI’s Community Vulnerability Compass (CVC), a non-medical drivers of health (NMDoH) data integration and visualization tool enabling deeper understanding of the context and complexities of the social barriers to health, access and well-being of Transplant Institute patients. The CVC uses 26 clinical and socio-economic indicators clustered into four thematic domains denoting the health, resiliency and economic vibrancy of neighborhoods. The first application of these innovative digital technologies and enriched data assets was the launch of the industry-leading Transplant Quality and Research DataMart, an important collaboration between University Health Transplant Institute and PCCI.
“With the rollout of PCCI’s Transplant Quality and Research DataMart, these projects will take just hours to complete. This reduced time to make data available to our fabulous team, in turn, will speed up our research and quality processes by enabling our physicians and staff to access data exponentially faster as they work to save more lives.” – Francisco G. Cigarroa, MD, Professor of Surgery and Director, Alvarez Transplant Center
In partnership with UT Health San Antonio, the University Health Transplant Institute is one of the top five U.S. transplant centers based on survival outcomes in kidney, liver, and lung transplantation. Its innovations in clinical practice and management have driven utilization of higher-risk donor organs and expanded opportunities for more patients to receive lifesaving transplantation. The Transplant Quality and Research DataMart will be able to place equitable data insights in the hands of research and care teams, while serving as a catalyst to new breakthroughs in understanding barriers and their impact to health, and ultimately providing higher quality of care to residents of Bexar County and beyond.
“We are proud to support University Health and its mission to provide high impact and innovative care,” said PCCI CEO, Steve Miff, PhD. “Our work will support University Health’s position as a leader in the transplant field with the implementation of a digital data environment and a transplant quality and research DataMart. This will allow the University Health Transplant Institute team to enhance and extend research and outcome studies and expand cross-industry collaborations. Adding CVC, our advanced NMDoH analytics tool, University Health will be better able to understand the NMDoH for their whole transplant population and better serve and provide enhanced access and support for their patients across the state.”
“Our Transplant DataMart is the first of its kind to use data from a large transplant program in a standardized cloud-based format by incorporating clinical metrics and non-medical drivers of health that are connected to a network of databases and other researchers across the world. This unique system will help us improve outcomes for transplant patients, perform advanced analytics, reduce barriers to care and increase grant and research opportunities to expand and share our work,” said Bryan Alsip, MD, Executive Vice President and Chief Medical Officer of University Health.
This partnership will help University Health foster additional grant and research opportunities by moving the organization into the Observational Health Data Sciences and Informatics (OHDSI) program. OHDSI is an international network of researchers and observational health databases with a central coordinating center housed at Columbia University. Integrating OHDSI, the OMOP Common Data Model, and the OHDSI software tools into the UH ISTHMUS™ ecosystem enables University Health teams’ access to the open community data standards, open-source software, and ways to apply scientific best practices to generate reliable clinical evidence.
Also, PCCI’s CVC will allow the University Health Transplant Institute to analyze a patient’s NMDoH to help make informed, equitable decisions. The CVC gives the team the ability to query a patient’s address to assess the NMDoH factors impacting that patient’s residential block group. This informs and enables more targeted screening questions and the collection of enhanced data to facilitate collaboration with community and health care organizations to support current and prospective patients throughout their transplant journey.
“University Health Transplant Institute has a 53-year history of cutting-edge innovation and superior survival rates. We are now one of the two largest living donor programs in the US and number one in survival. We also have the top survival and transplant rates for kidney and lung in our region including pediatrics. We have continually expanded access to our unique patient population through new medical techniques in lung, liver, and kidney transplantation and hepatocellular tumors and cancers,” said Francisco G. Cigarroa, MD, Professor of Surgery and Director, Alvarez Transplant Center, Malú & Carlos Alvarez Distinguished University Chair, and Ashbel Smith Professorship in Surgery.
“However, data projects to analyze and share our successes, can take us weeks or even months to complete. With the rollout of PCCI’s Transplant Quality and Research DataMart, these projects will take just hours to complete. This reduced time to make data available to our fabulous team, in turn, will speed up our research and quality processes by enabling our physicians and staff to access data exponentially faster as they work to save more lives. This in turn will lead to better outcomes and enhanced access to life-saving transplantation. This also allows us to share our successes with the transplant community around the world to make lives better,” Cigarroa added.
ABOUT UNIVERSITY HEALTH
University Health is the only locally-owned health system in San Antonio. For more than 100 years, University Health has been here to heal, improve health, train the next generation of medical professionals and ensure the people of San Antonio, Bexar County and South Texas have access to primary and advanced specialty care close to home. Specialized services include the region’s only Level I trauma center for both adults and children, and maternal and neonatal intensive care centers designated at the highest levels by the State of Texas. As the region’s only academic health system, University Health is a hub of innovation and discovery, committed to delivering patient-centered, culturally competent, high-quality and compassionate care, based on a strong foundation of outcomes‐based research and innovative teaching. Learn more at UniversityHealth.com.
About PCCI
The Parkland Center for Clinical Innovation (PCCI) is a not-for-profit, mission-driven organization with industry-leading expertise in the practical applications of artificial intelligence, machine learning and NMDOH data modeling to address the needs of vulnerable populations. PCCI started as a department within
Parkland Health and was spun out as an independent organization in 2012. PCCI strives to leapfrog the status quo by harnessing the transformative potential of data. Our unique capabilities allow us to provide innovative, actionable solutions that more effectively identify needs, prioritize services, empower providers, and engage patients.
North Texas Giving Day: Join us in our journey to bring health innovation to the most vulnerable communities
North Texas Giving Day, set for Sept. 19 but open to donations now, is a powerful opportunity to unite our community in supporting the causes we care about most. At PCCI, our team of clinicians and expert data scientists strive to support the health of vulnerable communities in North Texas through the responsible applications of AI and non-medical drivers of health (NMDoH) analytics. NMDoH are the conditions in the places where people live, learn, work and play (e.g., food insecurity, housing, transportation) that affect a wide range of health risks and outcomes. These external social, economic and environmental factors have been shown to be responsible for upwards of 80% of what keeps us healthy or, conversely, leads to illness and an impaired quality of life. As a non-profit, your support is critical to this mission.
Why support PCCI? You may have felt the impact of PCCI’s innovative AI and NMDoH programs during the COVID-19 pandemic when you learned about the spread of the infection through our neighborhoods. Or if you’ve checked the Dallas County Health & Human Services Department’s Pediatric Asthma Surveillance System dashboard―developed by PCCI― that offers insights into the asthma risks on your neighborhood. And you may know a pregnant woman who was able to bring their child to full term thanks to the Parkland Health’s Preterm Birth Prevention program powered by PCCI’s AI. We aim to ensure that each of our innovations are targeted to the unique needs of our community and equitably applied and support the most vulnerable in our neighborhoods.
Your Support is Critical in Creating Opportunities for Women in Technology
Benefiting the most from your support will be PCCI’s women in data science intern program, the Sachs Summer Scholars. PCCI developed this STEM-focused program to help open doors to women seeking careers in data science.This is an industry challenge as, according to Girls Who Code, from 1984 to today, the number of female computer science graduates dropped from 37% to 18% and computing degrees are less likely to be awarded to women in all racial and ethnic groups. These trends are taking place in spite of the fact that women outnumber men overall at universities. At PCCI we are committed to reversing this trend and improving diversity in the data science and technology industry all while focusing their contributions, efforts and learnings towards innovative, practical solutions supporting our local community.
Your support will enable PCCI to continue to provide unrivaled opportunities for undergraduate, graduate and doctoral female students from diverse backgrounds to work side-by-side with PCCI data scientists and clinicians and directly contribute to projects benefiting the community such as improving maternal health and pediatric asthma outcomes, lowering suicide risk, and developing a community surveillance system for diabetes and hypertension. In 2024, PCCI reported that 71.43% of participating interns were from diverse ethnicities. PCCI’s internship program helps these students to improve their self-confidence, hone their programming and analytics skills in order to open up greater career opportunities, fuel their passion for learning and helping their community, and build lifelong memories of meaningful accomplishments.
Our programs have proven to be cost effective, scalable, and successful. With your support, we will continue to explore new ways to apply AI solutions in collaboration with some of the top healthcare providers and public health organizations in the nation.
Early giving is open now, and every dollar counts. Your donation today will help us build momentum and maximize our impact on North Texas Giving Day. Together, we can create a brighter future for our community. Support PCCI in shaping the future of healthcare technology in North Texas.
Click here to donate now and be a part of the change!
PCCI introduces its 2024 class of Sachs Summer Scholars Interns
STEM focused program sets female students side-by-side with AI experts, data scientists and clinicians
PCCI’s summer intern program, Sachs Summer Scholars, Advancing Women in STEM and Technology Summer Internship, has begun, demonstrating PCCI’s ongoing commitment to improving gender diversity in the data science and technology industry. This program has become the one of the premier internship in North Texas that immerses students in meaningful, real word projects with actual impact. This includes providing each intern direct experience with innovative healthcare, groundbreaking artificial intelligence programs and Non Medical Drivers of Health projects. The aim is to support and promote practical applications of analytics, computing, and data science all while advancing the spirit of mentorship and advancement of female students.
The 2024 class of Sachs Summer Scholars includes seven women from diverse backgrounds, hailing from six different universities. Working side-by-side with PCCI clinical and data science experts to hone their programming and analytics skills while building life-long memories of meaningful accomplishments, the interns will work on core projects at PCCI including: disease surveillance systems, brain care predictive modeling, suicide risk screening, jail health and pediatric asthma risk prediction, to name a few.
This class will present findings based on their work with PCCI at a presentation on August 9th, at Pegasus Park.
The interns are, from left to right: Ozgur Aksoy, University of Texas – Dallas; Serap Ogut, Southern Methodist University; Autumn Carey Noon, Ohio State University; Bengisu Yarimbas, University of North Texas; Emily Thompson, Southern Methodist University; Ferona Bustani, University of Texas – Austin; Saniah Safat, University of Texas – Austin.
Suicide, a lack of psychiatric bed capacity, lack of access to psychiatry services, and other challenges are all too real in today’s healthcare environment. Using technology, however, to facilitate rapid diagnosis, treatment, and identification of resources is a welcomed relief to patients and clinicians alike. With a focus on various technologies, attendees will realize the difference that technology makes in the lives of patients and their families.
SPEAKERS:
Jacqueline Naeem, MD, Senior Medical Director at PCCI
While 80-85 percent of sepsis cases present within the first 48 hours of admission (ED), they have lower mortality (5-10 percent) as compared to 15-20 percent of cases that present later and have higher mortality (15-30 percent). To better (and earlier) identify sepsis cases not present on admission, at a large safety-net hospital, an end-to-end early sepsis prediction and response workflow was created in the inpatient setting. First, an ML model was built to predict the risk of a patient becoming septic in real-time. Next, the model baked into clinical workflows through FHIR APIs to make the model actionable at point of care. The model accesses EMR every 15 minutes and alerts the care providers when the risk exceeds a certain threshold, which can be tailored to local populations. Finally, an EHR-integrated decision support app (ISLET) was added to enable clinicians to easily view and understand model output to improve actionability. Prediction, alerting, visualizing the root causes and acting on the case completes the workflow. This full workflow has been running for thousands of patients every 15 minutes in the last year. This session will focus on the challenges, achievements and impact of this workflow on healthcare outcomes.
SPEAKERS:
George Oliver, MD, PhD, Vice President, Clinical Informatics at PCCI
Nainesh Shah, Assistant Professor, Health Informatician at Parkland Health
Yusuf Tamer, Principal Data and Applied Scientist at PCCI
The presenters built an AI- ML-driven pediatric asthma surveillance system (PASS) to monitor the clinical and social risk of pediatric asthma at the census tract level in Dallas County. First, they developed a novel AI/ML pediatric asthma risk index, combining clinical and social risk factors from multiple data sources to accurately predict census-tract risk of asthma-related emergency department visits and hospitalizations. Subsequent analyses identified actionable risk drivers which, combined with the novel asthma risk index, painted a wholesome, countywide picture of pediatric asthma risk disparities. PASS is an interactive, community-facing dashboard that maps and compares the distribution of the asthma risk index and other risk drivers across Dallas County. PASS is hosted on the Dallas County Health and Human Services website and is readily accessible to community stakeholders. Launched in January 2023, PASS was introduced to the community through training sessions and dissemination events to engage key stakeholders. PASS is being leveraged to advance health equity through diverse use cases ranging from environmental advocacy to city planning, clinical resources deployment, school-based interventions and corporate social responsibility. Lessons learned from PASS provide a blueprint for other scalable AI/ML-driven chronic disease surveillance systems such as diabetes and hypertension.
SPEAKERS:
Teresita Oaks, Director, Community Health Programs at Parkland Health
Yolande Pengetnze, MD, Vice President, Clinical Leadership at PCCI
Yusuf Tamer, PhD, Principal Data and Applied Scientist at PCCI
Occupational Safety and Health Administration (OSHA) defines workplace violence (WPV) as any act or threat of physical violence, harassment, intimidation or other threatening disruptive behavior occurring at work. Healthcare and social service workers are five times more likely to be injured than other workers and WPV rates continue to rise. Due in part to poor reporting systems, and the common misperception that violent events should be expected while working in healthcare, prevention measures rarely match the issue’s severity and often go unreported. This session will focus on efforts, in a large safety-net hospital, to address an important gap impacting WPV prevention efforts through the development of a predictive model to more accurately identify―in an inpatient healthcare setting―potentially violent patients, thus enabling healthcare workers to mitigate risks of impending WPV incidents.
SPEAKERS:
Karen Garvey, Vice President, Safety and Clinical Risk Management at Parkland Health
Alex Treacher, PhD, Senior Data and Applied Scientist at PCCI
Reshma Suresh, MS/MA, Data and Applied Scientist at PCCI
U.S. suicide rates increased by 27.6 percent over the past 15 years and suicide remains a leading U.S. cause of death, with 48,183 deaths in 2021, according to the CDC’s National Center for Health Statistics and the United Health Foundation. Development of evidence-based practices has dramatically increased over the past 20 years; however, suicide rates continue to increase in part due to broad variability in adoption of, and consistent adherence to, suicide prevention practices. As a vital first step in understanding suicide prevention from a population health perspective, and improving risk recognition for treatment application, a large safety-net hospital implemented a universal suicide screening program (SSP) in 2015, in which all patients ages 10 and older are screened for suicide risk during every provider encounter. This session will determine if the SSP reduces the number of patients falsely identified as not at risk of death by suicide in our cohort by linking mortality data to healthcare utilization data from five years pre- and post- SSP implementation. Despite suicide being a relatively low base-rate event (13-14/100,000 in the U.S.), the massive dataset size provides enough power for statistically meaningful changes to be detected.
SPEAKERS:
Jacqueline Naeem, MD, Senior Medical Director at PCCI
Alex Treacher, PhD, Senior Data and Applied Scientist at PCCI
PCCI Releases New Annual Impact Report Covering Highlights from 2023
Today PCCI has released its 2023 Annual Impact Report, demonstrating its value to the communities and individuals it serves.
To view and download the PCCI 2023 Annual Impact Report, click HERE.
The report offers insights into a few of the most impactful PCCI’s innovative programs, such as the launch of the Community Vulnerability Compass; our efforts to reduce the harm caused by pediatric asthma with the creation of the Pediatric Asthma Surveillance System; our innovative creation of AI/ML models to support trauma patients; and the work around the state to increase equity and access to healthcare through its Connected Communities of Care initiatives.
“Last year we saw PCCI evolve to support programs statewide with impactful innovations and collaborations that benefit residents in Dallas, Houston, Austin and San Antonio,” said PCCI CEO, Steve Miff, PhD. “We also joined leading national organizations via the Health AI Partnership to co-create and drive the ethical and meaningful applications of AI in clinical care and continue to be fully committed to helping revolutionize the way healthcare is delivered through the use of advanced data in clinical and community settings. This report gives you a peek into the broad swath of innovative work that PCCI does in support of our mission.”
About PCCI
PCCI started as a department within Parkland Health and was spun out as an independent, not-for-profit organization in 2012 to not only serve the needs of Parkland, but to also pursue additional transformative initiatives that could have a broader impact. PCCI remains tightly connected to Parkland Health, the Parkland Foundation and the Parkland Community Health Plan. Our collaborative work focuses on the needs of vulnerable populations across North Texas and beyond.
PCCI CEO featured at Xtelligent Healthcare Media’s 4th Annual Payer+Provider Virtual Summit
Watch the recording of PCCI President & CEO Steve Miff, PhD, at Xtelligent Healthcare Media‘s 4th Annual Payer+Provider Virtual Summit where he shared real-world examples and best practices for combining the right people, efficient processes, and advanced technology to address the needs of underserved individuals and populations.
From the program overivew:
Collaboration between providers and payers enables the pooling of resources, expertise, and data, fostering coordinated and efficient care for communities. This unified approach, especially in value-based care models, promotes preventive health measures, streamlines processes, and addresses holistic community health needs.
PCCI talks non-medical drivers of health data at Healthier Texas Summit
At the recent Healthier Texas Summit, Jacqueline Naeem, Senior Medical Director, Olayide Adejumobi, Associate Researcher and Guadalupe Negrete-lira, Manager, Connected Communities of Care, hosted an impactful 90-minute workshop. The session explored the potential for non-medical drivers of health (NMDOH)-related data to facilitate innovation between traditional healthcare settings and public health. During this workshop participants had the opportunity to share ideas on how to better integrate CHWs into healthcare systems, and improve collaboration.